Posted on January 14, 2022 View all news
Ed Wood, President, DUID Victim Voices

January 3, 2022
To – Senate Commerce, Science and Transportation Subcommittee
I am Ed Wood, founder of DUID Victim Voices, writing to correct misinformation you heard from Colorado Senator John Hickenlooper during the December 16th Commerce, Science and Transportation subcommittee confirmation hearing for Dr. Steven Cliff.
Senator Hickenlooper said “When we first legalized recreational marijuana in Colorado, which I opposed in the beginning, I thought there would be all kinds of increases in teenage driving, teenage consumption, frequency of use. We haven’t seen any of that—but we do recognize that we don’t have a good way to measure intoxication level.”
He then asked Dr. Cliff, “We use 5 ng of THC in the blood as the state standard. Are you willing to commit to working with this committee to develop a federal marijuana-impaired driving standard?”
Senator Hickenlooper was wrong on:
- The effect of marijuana legalization on Driving Under the Influence of Drugs (DUID),
- The effect of marijuana legalization on teenage marijuana use, and
- The wisdom of a marijuana impaired driving standard.
Following are data to prove these claims.
Driving under the influence of drugs (DUID)
Driving under the influence of drugs in Colorado, especially marijuana has increased substantially since legalized marijuana became effective in 2014. But polydrug impairment, led by marijuana combined with alcohol, is both far more common and growing more rapidly than impairment by marijuana’s D9-tetrahydrocannabinol (THC) only. Polydrug impairment is also much more dangerous than impairment by THC only.
Table 15 below shows the Colorado State Patrol citation trend by trooper’s assessment of the cause of DUI arrest. From 2014 (the date marijuana legalization became effective) to 2020, DUI citations involving marijuana increased from 12.0% to 31.4%. Marijuana only citations increased from 6.3% to 8.7%. Alcohol only now causes just over half of DUI citations.

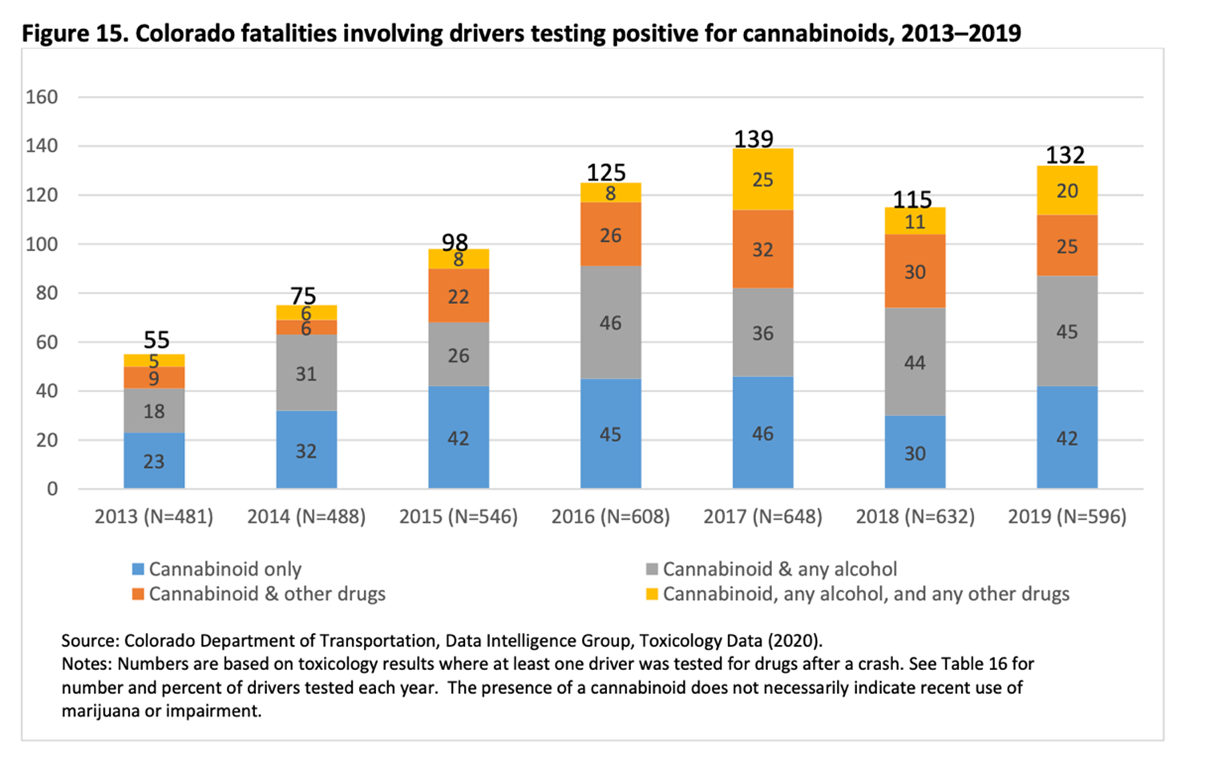
Figure 14 below goes beyond the trooper’s assessment of the cause, showing the tread of marijuana’s cannabinoid presence in fatal crashes.
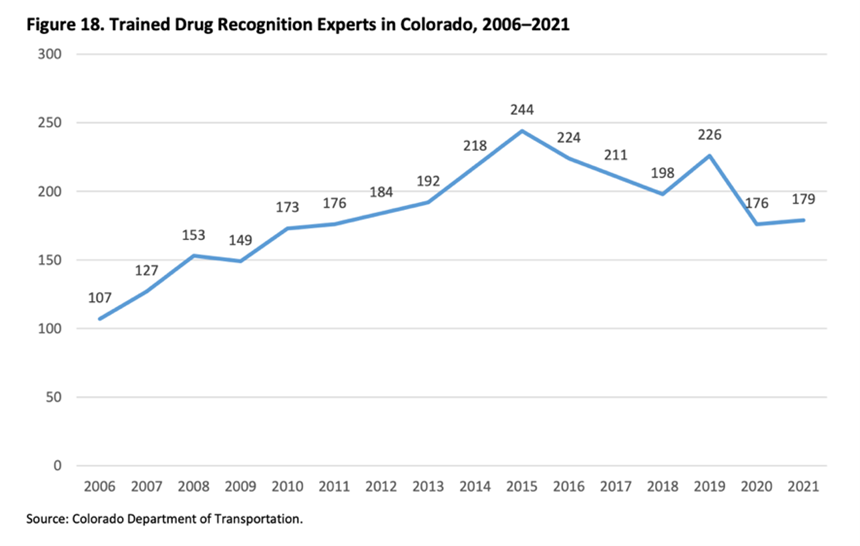
Colorado’s increasing DUID trend is not caused by more officers diligently detecting drugged drivers. In fact, the number of Drug Recognition Experts has declined since legalized recreational marijuana came into effect as shown below. Also, as can be seen in Table 15 on page 2, the number of citations of all types has been flat or even decreasing, and certainly not increasing:
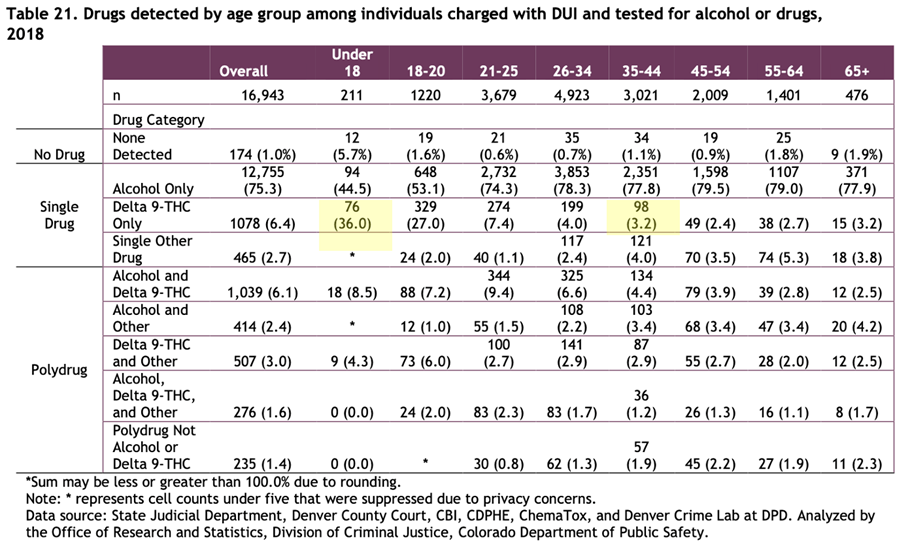
Teens have a substantially higher proportion of DUI arrests from marijuana’s THC than older drivers, and much less polydrug impairment than older drivers. For drivers under age 18, 36% of DUIs were due to THC and only 12.8% were polydrugs. For drivers 35-44, the percentages were 3.2% and 17.8% respectively.
Teen driving after using marijuana is particularly problematic and increasing rapidly. The biennial Healthy Kids Colorado Survey found that 54.4% of current teen marijuana users self-reported driving after marijuana use in 2019, up from 46.4% just two years earlier.
Beginning July 2019, the Colorado Bureau of Investigation toxicology laboratory began testing 100% of all blood samples submitted for DUI testing not just for alcohol, but for a full drug panel. The following table shows the results of the first year of that policy change. Positive THC cases outnumbered positive alcohol cases by 4,069 to 3,956.

The trend of increasing numbers of THC-positive DUI case filings keeps increasing year after year.

Teen marijuana use:
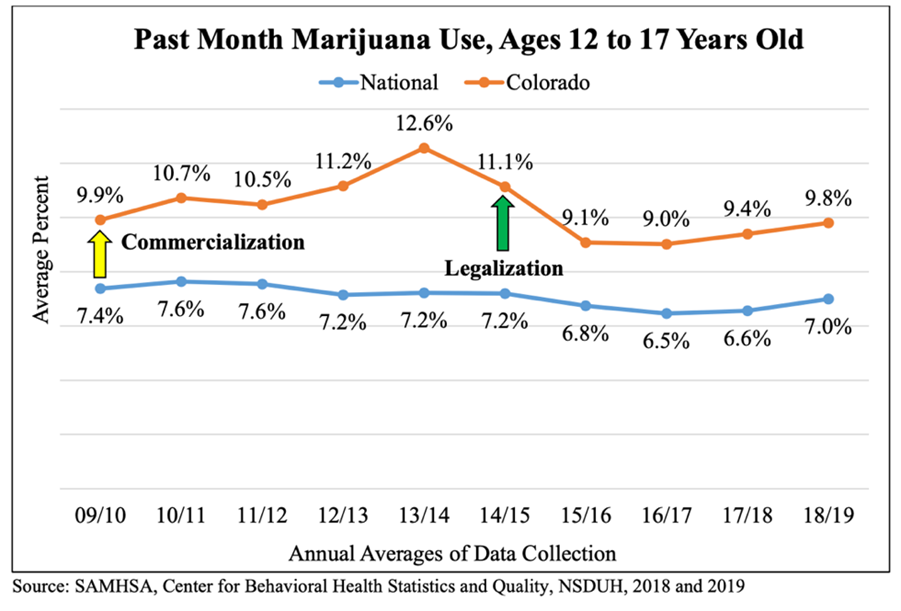
Colorado teens continue to use marijuana far more frequently than the national average, but there has been no consistent trend of increase, as Senator Hickenlooper noted.
Note: This chart shows past month use by students ages 12-17. Use rate by high school students is double the rate shown.
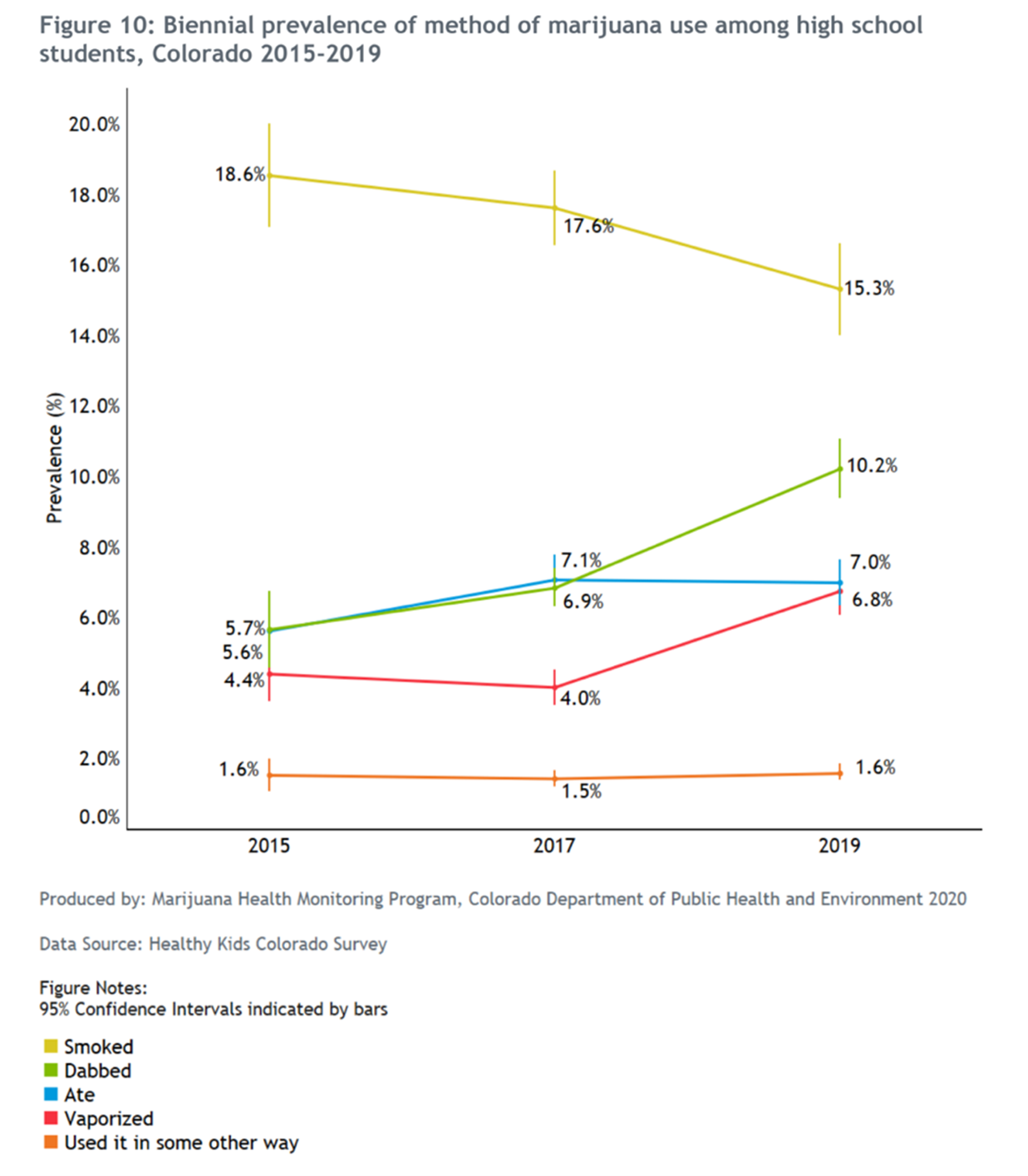
However, Colorado teens are increasingly using the drug in more highly concentrated forms – dabbing and vaping. High concentration marijuana preparations increase the risk of Cannabis Use Disorder (addiction), Cannabis Induced Psychosis, Cannabis Hyperemesis Syndrome, schizophrenia, and suicide. To address these known problems, the Colorado legislature this year restricted access to large quantities of high dose concentrates for resale but was unable to reach an agreement with the marijuana industry to cap the concentration (potency) of their drug products.
Marijuana impaired driving standard
The 2001 Department of Transportation Appropriations Act required states to establish alcohol per se levels no higher than .08 gm/dL or they would begin to lose highway construction funds. By 2004, .08 gm/dL BAC had become the national standard. Utah lowered its alcohol per se level to .05 gm/dLin 2018.
A BAC greater than .08 gm/dL (or above .05 gm/dL) does not prove that the driver was drunk. It merely proves the driver was in violation with the state’s DUI per se law. Sanctions for driving drunk and driving in violation of the DUI per se law are typically identical, so many people assume incorrectly that they mean the same thing.
It was relatively easy to gain acceptance of alcohol DUI per se legislation because of the high statistical correlation between a driver’s BAC and the risk of crashes, fatal or otherwise.
Alcohol is unique among the impairing drugs in having such a high crash risk correlation with drug content in the blood. There has been no other drug, including THC, for which a correlation has been demonstrated. For THC, not only is there no correlation whatsoever, we now understand the scientific reasons why no correlation can ever be shown, as explained on the next two pages.
Nevertheless, two states (Ohio and Nevada) have established 2 ng/mL as a THC per se limit in whole blood, and three states (Washington, Montana, Illinois) have established 5 ng/mL as a THC per se limit. Colorado established a THC 5 ng/mL permissible inference level, which simply means that the court may infer impairment if a driver’s blood THC content was at least 5 ng/mL and other evidence supports that inference.
Following are the reasons we assert that any non-zero THC per se level is contrary to science, common sense, and the lessons of experience.
DUID is not just about marijuana.
Just as DUI is not just about alcohol, DUID is not just about marijuana. From 2016-2018, Colorado forensic toxicology laboratories reported finding 86 impairing drugs in addition to alcohol and THC in the blood of drivers arrested for DUI.
Recognizing this fact, 16 states that have zero tolerance laws for drugs, specify a long list of drugs that are proscribed in drivers’ blood. Most, but not all those states include THC in their list. Three states that have non-zero per se limits for drugs include per se limits for 5-10 different drugs. Two of those states include THC on their list.
Marijuana is not just about THC.
The 2018 Farm Bill effectively legalized the sale of new psychoactive drugs derived from hemp. Drugs such as D8-THC, D10-THC, and THC-O-Acetate are now sold on the internet. All are psychoactive, none are on the Controlled Substance Schedule, and few states have made them illegal. A driving standard for marijuana’s D9-THC would not apply to these newer drugs.
Polydrug impairment makes individual drug per se limits less meaningful.
The high prevalence of polydrug impairment was shown on the table on page 3. In the three years Colorado has published comprehensive DUI data, 13.5% of all cases with toxicology results were polydrug cases, compared with 5.9% for THC only.
Virtually all research studies on polydrug impairment conclude that the impairing effects of multiple drugs is at least additive. This is especially true for the most common polydrug combination of THC plus alcohol. This means that if a driver tests below both the alcohol per se level and the THC per se level, that driver may be highly impaired.
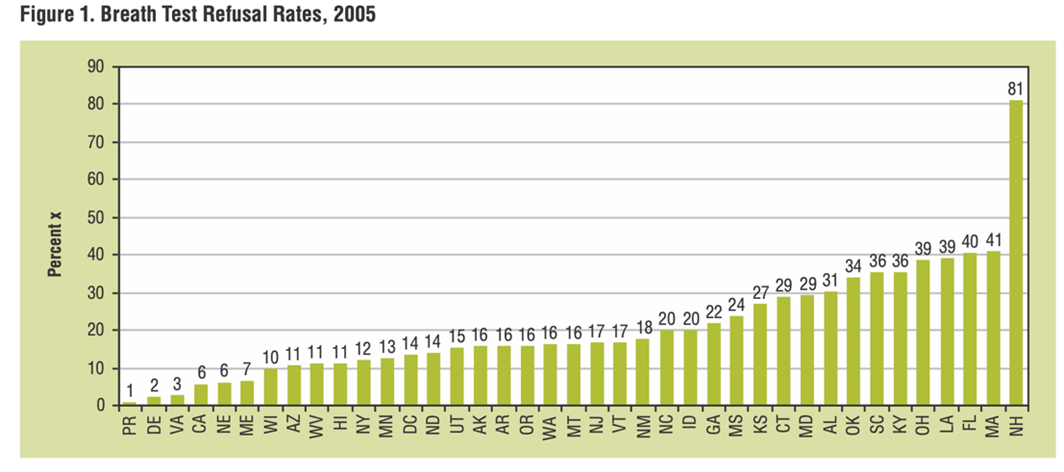
Per se limits are meaningless for drivers who refuse to submit to toxicology testing, Although all states have some form of implied consent requiring drivers to submit to toxicology testing when an arresting officer finds probable cause that the driver is impaired, many drivers refuse to comply. The proportion of drivers refusing to comply varies by state. In Colorado it is about one-third of all DUI arrests. Figure 1 below shows the refusal by state for breath testing. We have no data on refusals for drug testing, but we assume it might be higher.
There is no correlation between blood THC levels and the levels of impairment.
The scientific literature has published the following reasons why there is no such correlation:
- Blood THC levels do not track users’ subjective impairment ratings as blood alcohol levels do. During the first 30 minutes after THC consumption, blood THC levels decrease, while subjective “high” feelings increase.
- It typically takes about an hour to obtain a blood test sample after a routine traffic stop, two hours after an injury or fatal crash, and three hours if a warrant is required for a blood draw. The maximum THC level in blood has been shown to drop an average of 73.5% (3.3% – 89.5%) within the first 25 minutes after beginning smoke inhalation. Therefore, forensic blood assays cannot reliably reveal what the blood THC levels were at the time of the incident that led to the need for the assay.
- Smoking or vaping marijuana causes blood THC level to quickly rise, sometimes to over 100 ng/mL. The THC level then rapidly declines. This happens with both occasional and chronic smokers. But blood THC levels from marijuana edibles behave far differently. The blood THC level from consuming a common 10 milligram dose of a THC edible rises very slowly and does not rise to an average of 1 nanogram per ML, which is the limit of quantification for common forensic laboratories.
- The terminal half-life of THC determined with deuterium-labeled THC has been estimated to be 4.1 days. Therefore, low levels of THC can be found in the blood of chronic users for several weeks after ceasing all marijuana consumption, long after acute toxication has subsided. For that subset of users, any measurable blood THC level does not necessarily imply acute impairment.
- The partial tolerance of some chronic marijuana users to THC impairment is evidence that not only do blood THC levels have no correlation to the dose of THC consumed, but they also have no correlation to levels of impairment.
Those in the marijuana industry, fully aware of the above, claim that any THC per se level would be unjust because chronic users (including “medical” marijuana users) would be found guilty of DUI per se when they were not impaired. That is certainly theoretically possible, but we are not aware of any cases where it has happened. It should not happen, since a prosecutor must prove probable cause that the driver was impaired before a toxicology test can be admitted into evidence.
The flip side of the coin is that a severely impaired driver may be exonerated of DUI by testing below the THC per se level or permissible inference limit. Unlike the above speculative concern, this problem has been documented. The driver in Colorado’s Boulder County case 2016 CR 001454 was suspected of impairment by a Drug Recognition Expert (DRE) who requested that a second DRE perform a complete DEC evaluation. That second DRE found the driver to be unsafe to drive, and suspected marijuana as the cause. A blood sample was taken, and the driver’s blood had 1.5 ng/mL THC in it, consistent with the marijuana edible that the driver admitted to using prior to driving. The driver was not found guilty of DUI and was therefore sentenced to only 3 months in jail for carelessly driving over an 8-year-old girl on her way home from second grade, killing her.
Conviction rates are similar regardless of toxicology test availability.

Colorado’s 5 ng/mL permissible inference law isn’t working.
The above reasons show why THC per se limits are contrary to either science, common sense, or both. The biggest reason, however, is that experience proves the law simply doesn’t work. Colorado has two impaired driving misdemeanors. DWAI is defined as impairment to the slightest degree. DUI is defined as incapable of safe driving. The 5 ng/mL THC “legal limit” applies only to DUI. There is no THC per se limit or permissible inference level for DWAI. Conviction data from 2018 (the latest year for which we have data) revealed that the 5 ng/mL permissible inference level prevented DUI convictions of more than 90% of defendants who tested below 5 ng/mL even though most drivers under 5 ng/mL were impaired
| Charge category | # charged | # convicted | Conviction rate |
| DUI – 5.0 ng+ | 252 | 177 | 70% |
| DUI – 1.1-4.9 ng | 156 | 14 | 9% |
| DWAI – 5.0 ng+ | 467 | 464 | 99% |
| DWAI – 1.0-4.9 ng | 76 | 71 | 93% |
Although prosecutors may charge a defendant with both DUI and DWAI, each case is unique in the above table. There are no duplications.
Alcohol DUI charges resulted in convictions 96% of the cases when the driver’s BAC was at least .08 gm/dL and even 83% when no toxicology data were available. Yet THC DUI conviction rate was no higher than 70% when the driver’s blood exceeded the 5 ng/mL THC permissible inference level.
A full 74% of convictions for DUI caused by THC only were convictions for DWAI, even though there are no legal THC limits for DWAI. Most prosecutors prefer to charge defendants with either DWAI or DUI and DWAI, rather than just DUI. Charging only DUI may still be preferred by some prosecutors in cases of death or serious bodily injury, since vehicular homicide and vehicular assault caused by DWAI will not become unlawful until 2022.
Colorado is fortunate to have a DWAI statute that is not subject to the THC permissible inference law, or it would find that the overall conviction rate for driving under the influence of THC would be even lower than it already is.
Other states with THC per se laws may also have much lower DUI conviction rates for THC than for alcohol, but data like Colorado’s are not available to confirm that suspicion.
Conclusion
Senator Hickenlooper’s claims of marijuana’s safety reflect views of the marijuana lobby, not of reality. There are several rational actions Congress can and should take to deal with the rising incidence of drugged driving, but his plea for a federal marijuana driving standard is not one of them.
Sincerely,
Ed Wood
President, DUID Victim Voices